

Newsletter

July 2026
Don’t Just Count Visits. Capture What Matters.
Don’t Just Count Visits. Capture What Matters.
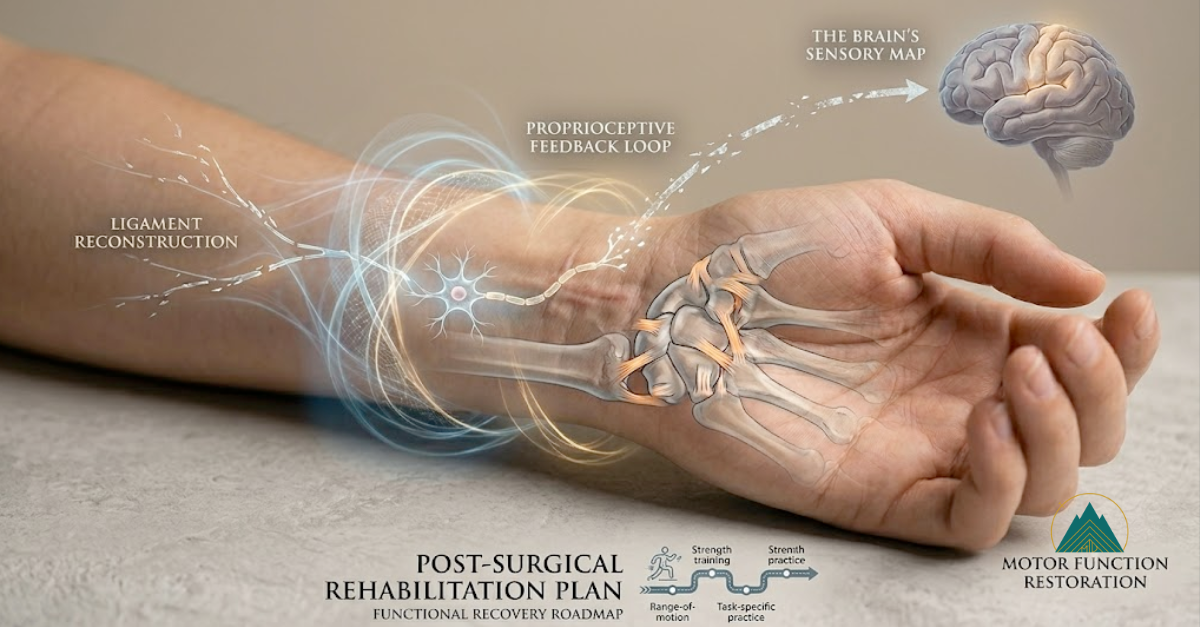
After a crash, it is easy to see the fracture and the scar. What you cannot see is how the wrist’s sensors and nervous system are struggling to relearn their job.
In a recent case involving a young woman with a complex multi‑carpal ligament reconstruction and wrist fracture, it could have been tempting to write “3 to 6 months of occupational therapy” and stop there. But realistic future care planning requires more.
Why proprioception changes the picture
The wrist is packed with receptors that tell the brain where the joint is in space, known as proprioception. When ligaments are torn and reconstructed, that feedback loop is disrupted. If you only plan for range of motion and strengthening, you miss the core problem.
Current research on wrist proprioception shows that targeted retraining improves neuromuscular control and function after ligament injury and reconstruction. That is why we explicitly included proprioceptive retraining in this future care projection instead of treating it as an optional extra.
How that changes the projection
For this client, our future care plan included:
Supervised occupational therapy for range of motion, proprioceptive retraining, progressive strengthening, and functional task training
A prolonged rehabilitation course that reflects the reality of multi‑ligament reconstruction and extensive adhesions
Custom orthotic fabrication and periodic adjustments as her recovery and functional demands evolve
In other words, not just “X weeks of therapy,” but a roadmap that reflects how clinicians actually treat this type of injury.
Why this matters for your cases
When we say we “capture what matters,” we mean:
We translate current rehabilitation science into concrete, case‑specific recommendations
We anticipate real‑world patterns such as plateaus and temporary setbacks that require brief returns to therapy
We account for evolving orthotic and functional needs, not just the early post‑operative phase
The result is a defensible, medically grounded projection that reflects how recovery really unfolds for your client.
If you are working on a case where the injuries and recovery do not fit a standard template, whether that involves multiple surgeries, lingering symptoms, or complex rehabilitation, I am always happy to be a resource.
P.S. If you find case‑based breakdowns like this helpful, follow me on LinkedIn for more posts. https://www.linkedin.com/in/darshika-goswami/

June 2026
The Delayed Connection: Traumatic Carpal Tunnel Syndrome
The Delayed Connection: Traumatic Carpal Tunnel Syndrome
We recently reviewed a case involving a client who struck the palm of her hand on the dashboard during a motor vehicle crash and later developed progressive numbness and tingling symptoms in that same hand. Our causation report addressed a central medical question: whether that type of blunt hand and wrist trauma could plausibly contribute to the later development of carpal tunnel syndrome.
In this matter, our report connected three key points:
-the dashboard impact to the palm
- published support that palmar force can raise carpal tunnel pressure
-inflammatory process that can help explain gradual symptom progression over time
By spelling out both the biomechanics and the slow-developing tissue response, the report made the timing medically understandable without overstating the science.
The value of a strong causation report is not just the conclusion, but the clarity of the explanation: mechanism, literature support, and a timeline that makes medical sense.
The Takeaway
A condition does not have to be obvious on day one to be real, important, or medically significant.
Some post-traumatic problems emerge gradually, and when they are finally identified, they can reshape the entire medical analysis, from treatment planning to future care needs.
That is the value of thoughtful MD-led review: seeing what may have been missed, explaining why it matters, and supporting the case with clear medical reasoning.
Let’s Talk About Your Case
Whether you need:
✅ A quick medical read
✅ A focused opinion letter
✅ Or full case strategy support
I’m happy to talk through how we can help.
— Darshika Goswami, MD
Pacific Northwest MD Legal Consulting
📧 info@pnwmdlegal.com
📞 (503)‑308‑9186

May 2026
When the Pain Does Not Match the Injury
When the Pain Does Not Match the Injury
A fracture heals. The incision closes. Imaging looks acceptable. But sometimes the pain does not follow the expected course.
We reviewed a case that began with a penetrating extremity injury in a man with diabetes, followed by wound infection, cellulitis, and multiple surgical procedures. Early on, the symptoms looked relatively predictable, with pain and swelling centered at the wound site and involving the nearby muscles and tendons.
Over time, however, the clinical picture changed. The pain worsened, spread beyond the expected pattern, eventually manifesting neurological features that no longer fit a routine recovery.
The Disproportionate Shift
This shift is critical. The reported pain became disproportionate to the physical exam and adopted a regional distribution rather than following standard nerve pathways. Other red flags appeared: the client described alternating sensations of heat and cold, and the skin fluctuated between being abnormally dry and excessively sweaty—classic signs of the autonomic dysfunction seen in Complex Regional Pain Syndrome (CRPS).
The Danger of "Diagnostic Anchoring"
This is why CRPS is often missed early. Some of the most important signs can be intermittent. By that time, the record begins to suggest that the pain no longer matches the original injury, and the case may already be anchored to an incomplete diagnosis.
Takeaway
This is part of the value of careful MD-led medical review: identifying when the recovery pattern no longer fits, recognizing overlooked pain syndromes, and translating that progression into a clear, medically supported opinion. If your case involves pain that seems out of proportion to the injury or recovery that no longer makes medical sense, reach out to discuss whether a closer review may be warranted.
Let’s Talk About Your Case
Whether you need:
✅ A quick medical read
✅ A focused opinion letter
✅ Or full case strategy support
I’m happy to talk through how we can help.
— Darshika Goswami, MD
Pacific Northwest MD Legal Consulting
📧 info@pnwmdlegal.com
📞 (503)‑308‑9186
April 2026
When a “Normal MRI” Doesn’t Explain Severe Post-Crash Headaches
When a “Normal MRI” Doesn’t Explain Severe Post-Crash Headaches
We recently reviewed a case involving a mid-career professional whose recovery had stalled after a motor vehicle crash.
His biggest problem was not neck pain.
It was his inability to tolerate a computer. After about 2 hours of screen time, he developed severe headaches that made it difficult to do his job.
The early medical records focused on the expected diagnoses: mild concussion and cervical whiplash.
His brain MRI was normal, and the medical records began to frame his symptoms as a typical post-concussion complaint.
But a closer review pointed to something often overlooked after trauma:
visual focusing dysfunction.
The Medical Connection
In this case, we were able to support the causation of the visual disturbance and headaches through two overlapping mechanisms:
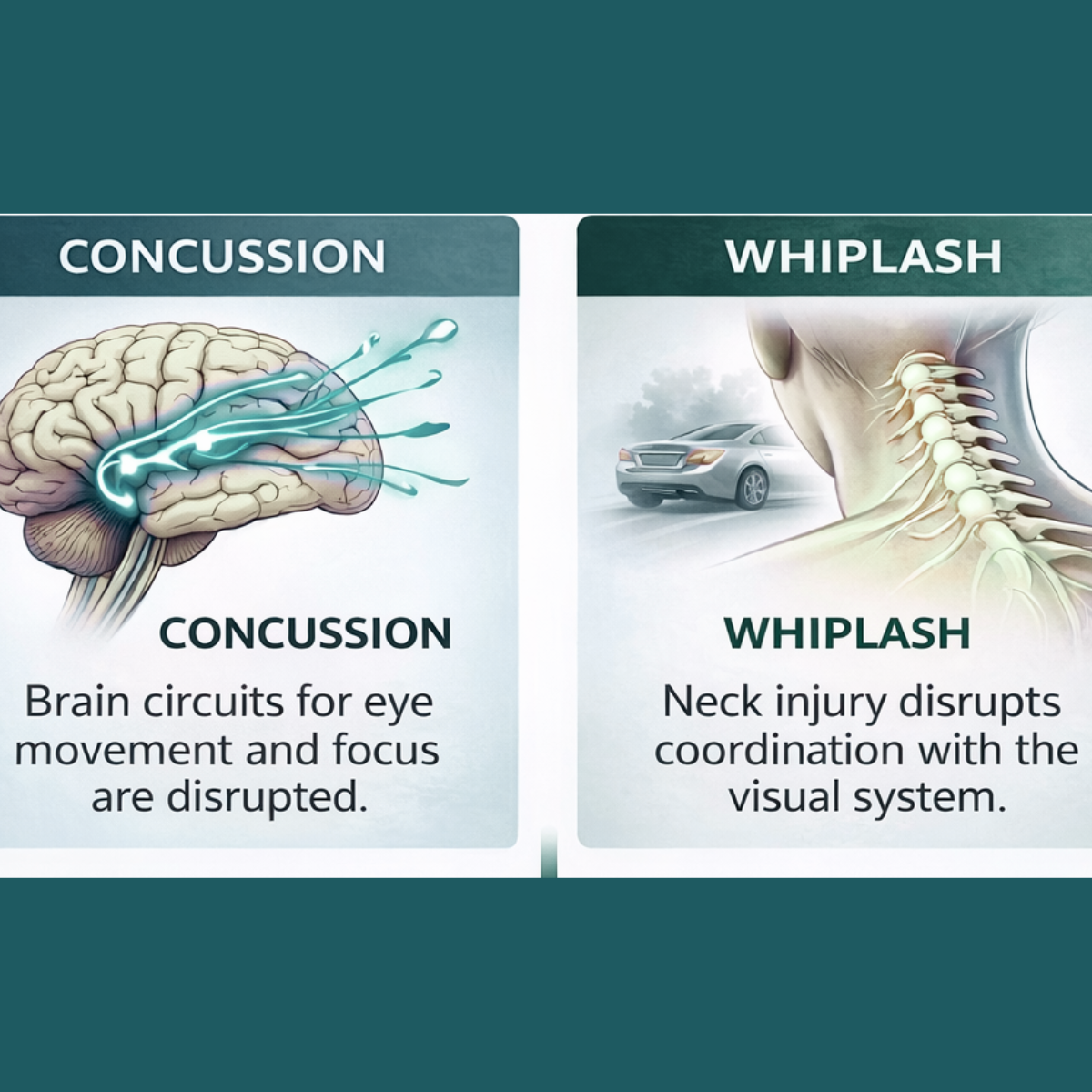
1. Concussion.
A mild traumatic brain injury can disrupt the brain circuits responsible for coordinating eye movements and visual focus.
2. Whiplash.
A cervical spine injury can disturb the neck’s proprioceptive system, which helps the brain coordinate head position with eye tracking.
When these systems are affected, patients often develop:
• headaches triggered by reading or screen use
• blurred or double vision
• rapid eye fatigue
• difficulty sustaining near work
These symptoms are well documented in the medical literature after concussion and cervical trauma, yet they are frequently missed unless the visual system is specifically evaluated.
How This Changed the Case
Identifying the actual causation of his symptoms changed the medical narrative.
Instead of a vague post-concussion complaint, the case now had a clear diagnosis and a medically supported pathway for treatment.
Our future care and cost projection included:
• neuro-optometric rehabilitation therapy
• specialized corrective lenses
• long term follow up with the eye clinic
The Takeaway
Not every meaningful post-traumatic condition appears on imaging or gets recognized early.
When these conditions are identified, the medical picture often changes, including treatment recommendations, future care, and projected costs.
This is part of the value of careful MD-led medical review: recognizing overlooked injury mechanisms and translating them into clear, medically supported opinions.
If a client continues to struggle with headaches, visual fatigue, or screen intolerance after concussion or whiplash, the record deserves a closer look.
Let’s Talk About Your Case
Whether you need:
✅ A quick medical read
✅ A focused opinion letter
✅ Or full case strategy support
I’m happy to talk through how we can help.
— Darshika Goswami, MD
Pacific Northwest MD Legal Consulting
📧 info@pnwmdlegal.com
📞 (503)‑308‑9186
March 2026
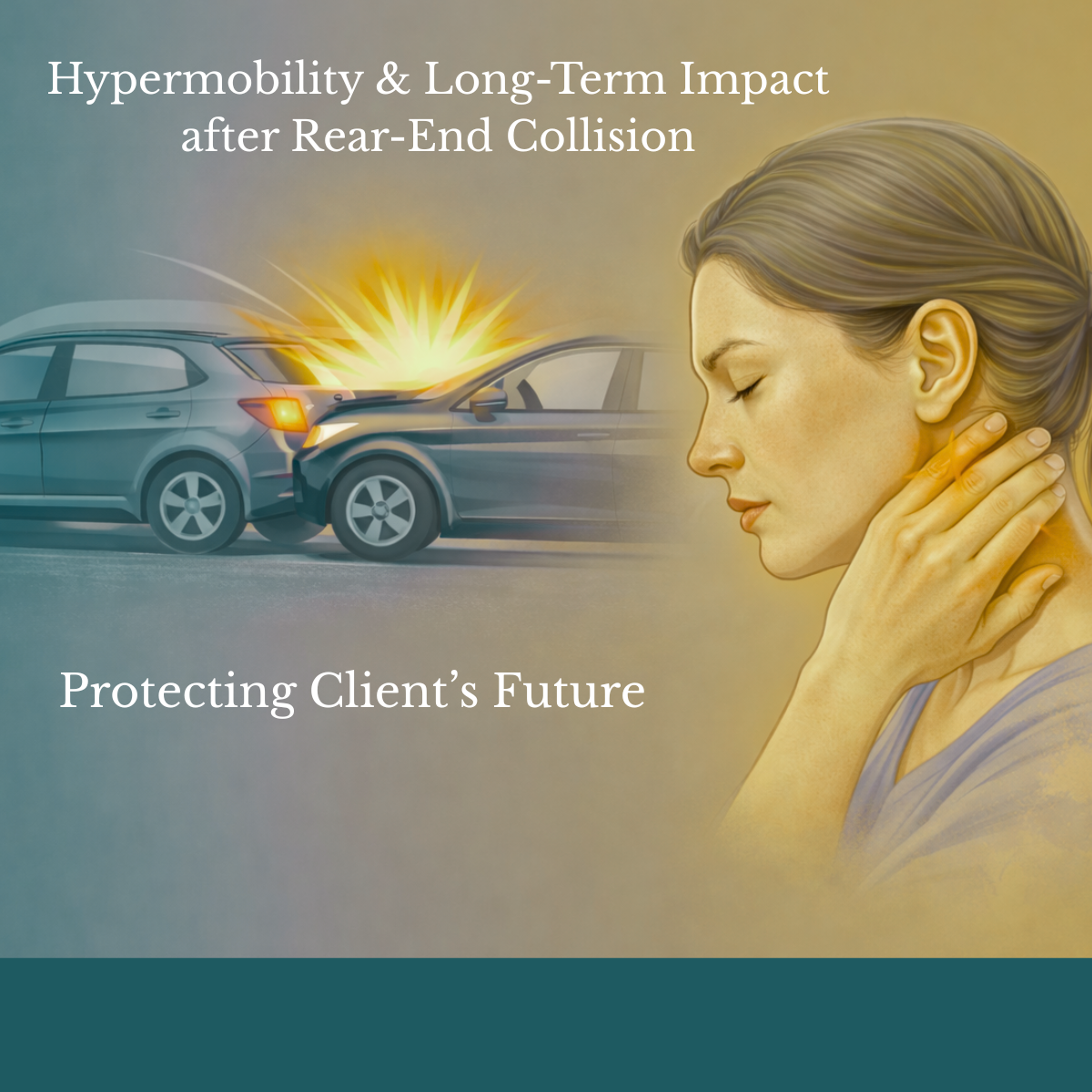
Hypermobility & Long-Term Impact after Rear-End Collision
When “Young and Healthy” Isn’t the Full Story
We were recently consulted on a case involving a 20-year-old rear-ended in a motor vehicle collision.
He presented with neck pain and headaches.
No fracture.
Discharged medically stable.
On paper, it looked like a routine soft-tissue case.
But this client has baseline hypermobility, meaning increased ligamentous laxity that permits greater motion in the cervical spine under load.
Hypermobility does not create injury.
It changes how force is absorbed and how the body heals.
In a 20-year-old, that distinction matters.
The 58-Year Horizon
At age 20, even mild cervical instability can translate into:
Ongoing physiatry oversight
Intermittent physical therapy over decades
Medial branch blocks and possible radiofrequency ablation
PRP injections
Periodic neurosurgical monitoring
Repeat imaging as symptoms evolve
This is not speculative.
This is trajectory from a medical perspective.
How This Adds Value to Your Case
This is about accurately modeling the medical progression set in motion by the accident.
Our future care and future cost projections account for:
Underlying biological vulnerability
Adjacent segmental disease
Long-term monitoring and intervention
Frequency, duration, and realistic cost benchmarks
This is another way we add value to your cases, by identifying long-tail medical exposure before it is overlooked.
If you are evaluating a young client whose recovery is not tracking the way it should, we are happy to review the file and provide a focused assessment.
Let’s Talk About Your Case
Whether you need:
✅ A quick medical read
✅ A focused opinion letter
✅ Or full case strategy support
I’m happy to talk through how we can help.
— Darshika Goswami, MD
Pacific Northwest MD Legal Consulting
📧 info@pnwmdlegal.com
📞 (503)‑308‑9186
February 2026
When Trauma Triggers Death in Patients with Pre-Existing Heart Disease
When Trauma Triggers Death in Patients with Pre-Existing Heart Disease
February is American Heart Month, which makes it an appropriate time to revisit a recurring issue in personal injury cases: how pre-existing heart disease is often treated as a stopping point rather than the start of a proper causation analysis.
We recently consulted on a case involving a high-impact auto collision. The client sustained severe traumatic injuries, including multiple rib fractures, leg fractures, and a partially amputated foot. He was airlifted to the hospital and died shortly after arrival in the emergency department.
The county coroner attributed the death to heart failure secondary to severe coronary artery disease, describing the automobile accident as a “possible contributory factor.” That language is common, and it is often where insurers attempt to discount the role of trauma.
From a medical standpoint, this framing is incomplete.
Severe trauma produces an intense physiologic stress response, including a surge of catecholamines (organic compounds, specifically monoamine neurotransmitters and hormones, that play a critical role in the body’s acute "fight-or-flight" stress response). In patients with advanced coronary artery disease, this response can acutely narrow already compromised vessels while increasing myocardial oxygen demand. The result can be sudden cardiac failure that would not have occurred at that time but for the traumatic event.
In this context, heart disease represents vulnerability, not inevitability. The trauma serves as the precipitating event.
This mechanism is well supported in the medical literature, which consistently shows higher mortality rates following major trauma in patients with pre-existing cardiac disease, particularly when multiple cardiac risk factors are present. These deaths are temporally and biologically linked to the traumatic injury rather than occurring independently of it.
As we summarized in our analysis:
Stating that a patient died of heart failure due to coronary artery disease on the day of a massive auto accident is like stating someone died of “lack of oxygen” without mentioning they drowned.
The heart disease was the “water” (the vulnerability), but the auto accident was the “drowning” (the precipitating event).
When a client has underlying heart disease, the key medical question is not whether the disease existed, but whether the trauma triggered the fatal event. That distinction is easiest to establish when it is addressed early, before the medical record collapses causation into a single diagnosis.
This situation is another example of how we can assist you with all the medical issues in your cases and occasionally find previously undiagnosed medical damages.
Let’s Talk About Your Case
Whether you need:
✅ A quick medical read
✅ A focused opinion letter
✅ Or full case strategy support
I’m happy to talk through how we can help.
— Darshika Goswami, MD
Pacific Northwest MD Legal Consulting
📧 info@pnwmdlegal.com
📞 (503)‑308‑9186
January 2026
Can a Treating Doctor’s Medical Opinion on Causation Be Incorrect and Potentially Hurt Your Case?
Can a Treating Doctor’s Causation Opinion Be Wrong and Hurt Your Case?
This Month’s Case: When Early Input From a Physician Consultant Changes the Trajectory
We were recently asked to consult on a case that highlights a crucial question for attorneys handling injury claims:
What happens when the treating physician gets the causation wrong?
The Story:
A 49-year-old woman working retail had multiple boxes fall off a shelf, striking both legs, worse on the left. She was able to walk afterward and didn’t seek immediate care. Over the next three weeks, however, her left calf developed persistent aching, then mild swelling, and finally became painfully swollen, prompting an ER visit.
Diagnosis: acute deep vein thrombosis (DVT) in the left popliteal vein (behind the knee).
Treatment: standard anti-coagulation and follow-up care.
This is where the medical narrative diverged.
The patient had also been under the care of a gynecologist for large uterine fibroids, and during a routine visit (coincidentally, the same week she was diagnosed with DVT), the gynecologist suggested her clot was caused by pelvic vein compression from the fibroids. The hematologist agreed, referencing the gynecologist’s note and ruling out inherited clotting disorders.
The work injury was not mentioned.
When she applied for workers’ compensation, she pointed to the obvious timeline: trauma ➝ lingering pain ➝ swelling ➝ clot.
But now, the medical record contained two alternate opinions, neither of which accounted for the workplace trauma. That could have jeopardized the claim.
The Analysis: Medical Literature Tells a Different Story
As physician consultants, our role is not to override treating doctors but to ground causation in anatomy, mechanism, and evidence-based reasoning. Here’s what we found:
1. Anatomic Inconsistency
Fibroids may cause DVT, but only when very large, and usually in the pelvic or proximal femoral veins.
A popliteal vein DVT (behind the knee) is anatomically inconsistent with fibroid-related compression.
Conclusion: The proposed mechanism doesn’t align with known patterns of fibroid-related DVT.
2. Trauma Is a Well-Established Risk
Blunt leg trauma is a strong transient risk factor for DVT, particularly when deep tissue is involved.
Injury causes vascular endothelial damage, triggering clot formation.
Conclusion: The trauma mechanism fits the known pathophysiology of post-traumatic DVT.
3. Timeline Consistency
Trauma-related DVTs typically develop within 2–3 weeks, precisely what occurred here.
The progression from calf ache ➝ swelling ➝ clot is classic.
Conclusion: The temporal pattern supports a trauma-related DVT.
4. Fibroid-Associated DVT Is Exceptionally Rare
These cases are so uncommon that they’re often published as case reports.
Increased incidence appears only when uterine weight exceeds 1,000g—which was not the case here.
Conclusion: Fibroid-related DVT was statistically and clinically unlikely.
The Timeline Told a Different Story
The client, however, recognized a clear sequence: leg trauma followed by persistent pain, swelling, and eventual clot formation and believed her DVT was work-related. She filed a Workers’ Compensation claim, asserting that the clot stemmed from her on-the-job injury.
Why This Matters for Attorneys
This case underscores a critical point:
Treating physicians may mean well, but their causation opinions can be wrong, and that can hurt your case.
In this situation:
The anatomic location (popliteal vein)
The injury mechanism (blunt leg trauma)
The timeline (3 weeks to thrombosis)
…all point toward a work-related trauma as the cause, not uterine fibroids.
Our detailed medical review, complete with literature citations, gave the attorney the evidence needed to challenge the treating physician's narrative and support the client’s claim.
Let’s Talk About Your Case
Whether you need:
✅ A quick medical read
✅ A focused opinion letter
✅ Or full case strategy support
I’m happy to talk through how we can help.
— Darshika Goswami, MD
Pacific Northwest MD Legal Consulting
📧 info@pnwmdlegal.com
📞 (503)‑308‑9186
December 2025
Can Trauma Precipitate Fibromyalgia?
Can Trauma Precipitate Fibromyalgia?
Pacific Northwest MD Legal Consulting Medical Perspective
When a 39-year-old woman was hit by a drunk driver on the driver’s side of her vehicle, she didn’t think the injuries were serious. She was seat-belted, the airbags didn’t deploy, and X-rays in the ER were negative. She was discharged with a diagnosis of soft tissue strain.
But weeks later, her pain hadn’t resolved. It had spread from her neck and chest to her shoulder and upper back. Physical therapy worsened her symptoms. MRI imaging was unremarkable. A bone scan later showed mild increased uptake in the clavicle and upper chest, but still no structural damage.
Eventually, she was referred to a rheumatologist, who diagnosed fibromyalgia, a chronic pain condition that appeared to be precipitated by the collision.
Her symptoms now included widespread pain, fatigue, “fibro fog,” and significant functional decline. One year post-collision, she remained symptomatic and struggled with daily activities and work.
Medical Insight: When Trauma Triggers Fibromyalgia
Fibromyalgia is not a structural injury. It’s a disorder of central pain processing, involving:
Neurochemical imbalances (e.g., low serotonin, norepinephrine, dopamine)
Central sensitization — where normal sensations become painful (allodynia)
Disrupted pain inhibition — the nervous system amplifies pain signals instead of filtering them
Although its exact cause remains unclear, physical or emotional trauma can unmask or trigger fibromyalgia, especially in individuals with predisposing factors.
In this case, persistent pain following trauma, negative imaging, and evidence of localized inflammation (bone scan) aligned with early central sensitization, a known precursor to fibromyalgia.
Why This Matters in Personal Injury Cases
Fibromyalgia often presents without objective findings but that does not mean the condition is unfounded. Understanding how trauma can initiate central pain syndromes is essential in evaluating:
Causation
Credibility of symptoms
Long-term prognosis and damages
The absence of MRI or CT abnormalities doesn’t negate real impairment, especially when the timeline aligns and other causes have been excluded.
The Takeaway
In personal injury and disability cases, fibromyalgia can be both real and trauma-induced.
A clear understanding of central pain mechanisms, paired with a detailed clinical timeline, helps attorneys:
Recognize when fibromyalgia may be causally linked to an event
Support claims in the absence of structural damage
Articulate functional impairment in a language that holds up medically and legally
Need help reviewing a case involving fibromyalgia, chronic pain, or unclear imaging findings?
Let’s talk. Early physician input can make a critical difference.
Let Us Know How We Can Help You
